Why Homecare in India Needs Its Own “Stage 7” Moment
A White Paper on Homecare Competency, Trust Maturity, and System Design
1/26/20265 min read
Why Homecare in India Needs Its Own “Stage 7” Moment
January 25, 2026
Designing Healthcare at Home Around Its True First Principle
Executive Summary
Healthcare at home is expanding at unprecedented speed. Capital, technology, and policy attention are converging on the sector, promising a future where more care moves out of hospitals and into living rooms. Yet beneath this momentum lies a persistent discomfort that families struggle to articulate but experience daily.
Despite remote monitoring devices, telehealth platforms, compliance frameworks, and digital dashboards, families continue to feel the need to watch closely. They monitor caregivers, call supervisors frequently, and hesitate to step away for long. This behavior is not irrational. It is a rational response to systems that have not yet earned deep trust.
This white paper argues that the core constraint in healthcare at home is not technological capability or regulatory alignment. It is the absence of a shared framework that defines trust maturity — a way to distinguish between organizations that merely deliver services and those that can be depended on under real-world conditions.
Drawing inspiration from the HIMSS EMRAM framework, which transformed how hospitals approached digital maturity, this paper introduces Homecare Competency Levels (HCL 1–7). Unlike hospital maturity models that focus on system adoption, HCL focuses on how reliably trust is produced, particularly through caregivers operating alone in unpredictable home environments.
At the highest levels of maturity, technology does not impress families because it is rarely noticed. Caregivers are clinically capable, technically fluent, and system-supported. Escalations are rare, continuity is strong, and families experience something far more valuable than visibility — peace of mind.
The Question Families Never Stop Asking
Families rarely interrogate providers about their technology stack. They do not ask which remote monitoring vendor is deployed, whether dashboards are AI-enabled, or how data governance is structured. These questions belong to industry conferences, not kitchens and bedrooms.
What families ask, often silently, is far simpler and far heavier:
If I am not watching, will care still happen the right way?
This question is not philosophical. It is practical. It determines whether families can go to work, sleep through the night, or leave town for a day. When the answer is uncertain, families compensate by staying involved, checking in frequently, and intervening early. No amount of technology can override this behavior if trust has not been earned.
This paper is built around that question. It treats trust not as a brand attribute or emotional outcome, but as an operational achievement that can be designed, measured, and scaled.
Why Homecare Needs Its Own “Stage 7” Moment
During years of engagement with HIMSS USA and service on the HIMSS Global Health Education Committee, one pattern became unmistakably clear. Hospitals did not become safer or more dependable simply because they purchased electronic medical records. They became dependable when those systems were embedded deeply enough into clinical workflows that physicians trusted them during moments of pressure.
The EMRAM framework provided hospitals with a shared language of maturity. At EMRAM Level 7, hospitals reach a stage where digital systems are no longer adjuncts but integral infrastructure. Data flows reliably, decision support is available in real time, and clinicians trust the system enough to depend on it rather than work around it.
The defining feature of EMRAM Level 7 is not sophistication. It is reliability under stress.
Homecare today operates without an equivalent maturity lens, despite facing even greater variability and risk. Care is delivered in uncontrolled environments, often by a single caregiver, without the immediate backup of institutional supervision. Families assume emotional and practical risk every day, yet the sector lacks a structured way to define what dependable homecare actually looks like.
The insight was unavoidable: if hospitals needed a maturity model to earn trust, homecare needs one even more. Homecare Competency Levels (HCL) were conceived to fill that gap.
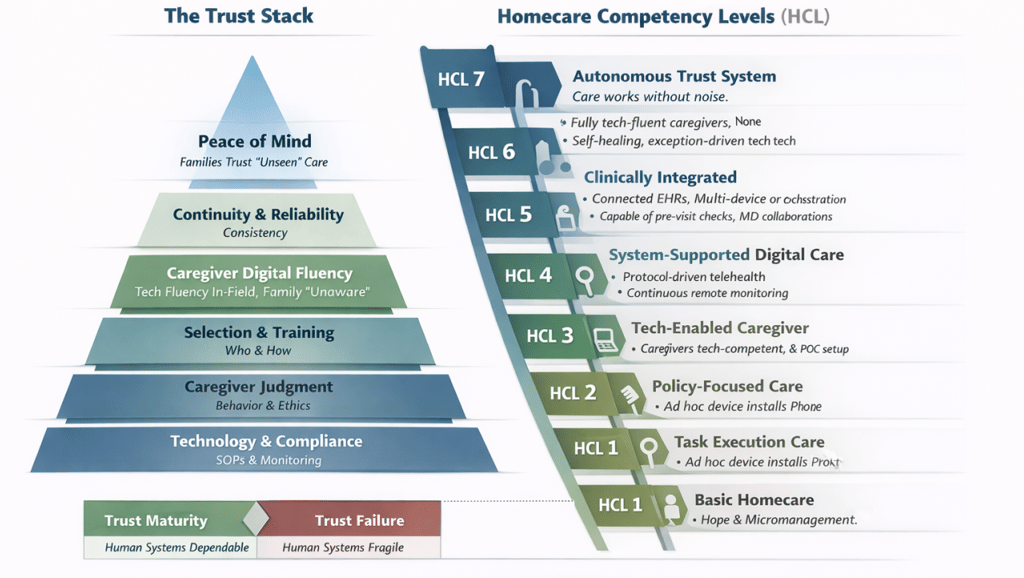
Trust Is Not a Feeling — It Is a Stack
Trust in healthcare at home does not emerge from a single intervention. It is the result of multiple layers working together, each reinforcing the next. Weakness in any layer undermines the entire structure, no matter how strong the others may be.
This layered model is referred to here as the Trust Stack.
At the foundation lies technology and compliance. Documentation, SOPs, regulatory adherence, and monitoring tools provide baseline safety and visibility. They are essential, but they do not, by themselves, produce trust. In many cases, they merely expose its absence.
Above this sits caregiver judgment — the ability to apply rules with context, manage ethical dilemmas, and respond calmly to uncertainty. No system can compensate for poor judgment in a private home setting.
Judgment, however, does not emerge spontaneously. It is shaped through selection and training, which determine who is allowed into homes and how their behavior is reinforced over time. Most large-scale homecare failures trace back not to intent, but to weak selection and insufficient behavioral training.
A critical and often underappreciated layer is caregiver digital fluency. At scale, caregivers must be able to independently set up and operate remote monitoring devices, enable full telehealth sessions, and manage point-of-care devices without transferring anxiety to families. When caregivers lack this fluency, technology becomes a source of friction rather than reassurance.
When these layers are strong, continuity and reliability emerge. Care becomes predictable, escalations decrease, and families begin to relax their oversight. Over time, the outcome is peace of mind — not as a promise, but as a lived experience.
See content credentials
Homecare Competency Levels - HCL 1-7
Homecare Competency Levels (HCL 1–7)
Homecare Competency Levels describe how trust maturity evolves as systems replace heroics.
HCL 1 represents task-based care, where outcomes depend almost entirely on individual caregivers. Technology is absent or unused, and families compensate by constant vigilance.
At HCL 2, basic processes exist, but supervision is reactive. Technology may be present, but caregivers rely heavily on families or supervisors to make it work. Trust remains fragile.
HCL 3 introduces digitally assisted caregivers. They can capture vitals, assist with teleconsultations, and operate basic point-of-care devices. Trust improves, but remains individual-dependent.
HCL 4 marks the inflection point. Caregivers are formally trained and certified in remote monitoring setup, alert handling, telehealth session facilitation, and independent device operation. Technology becomes operational rather than experimental, and families begin to step back.
At HCL 5, systems support caregivers proactively. Predictive escalation, tech readiness checks, and clear failure protocols reduce surprises. Trust shifts from individuals to systems.
HCL 6 integrates homecare into the broader clinical continuum. Caregivers act as extensions of hospital teams, and data flows reliably across settings. Institutional confidence emerges.
Finally, HCL 7 represents trust embedded at scale. Care quality is independent of individual actors. Technology is largely invisible. Families stop monitoring not because they are told to, but because experience has taught them they no longer need to.
Why Technology Alone Keeps Failing
Many homecare organizations assume that visibility creates trust. In practice, excessive visibility often increases anxiety. Dashboards multiply, alerts escalate, and families feel compelled to intervene.
This is not a technology problem. It is a maturity problem.
Technology amplifies the human system it rests upon. When caregiver competency and system design are weak, technology exposes fragility. When they are strong, technology fades into the background, doing its work quietly.
Reframing Excellence in Healthcare at Home
True excellence in homecare is not measured by feature lists or compliance scores. It is measured by whether families can delegate care without constantly supervising it.
Just as EMRAM reframed hospital excellence around dependable systems rather than digitization alone, HCL reframes homecare excellence around trust that holds under real-world pressure.
The most mature homecare organizations are not loud. They are calm. Their systems absorb variability instead of transmitting it to families.
Conclusion: Trust Is the Real Infrastructure
Healthcare at home is not a decentralization of hospitals. It is a delegation of responsibility, judgment, and vigilance into private spaces.
Organizations that treat trust as infrastructure — designed deliberately, layered carefully, and reinforced consistently — will define the future of the sector. Others will continue to add technology while wondering why anxiety persists.
The Homecare Competency Levels framework offers a practical path from ad hoc care to trust-embedded systems. It does not promise perfection. It promises reliability — the kind that allows families to step away and live their lives.
When that happens, healthcare at home finally becomes what it was always meant to be.